GM E-log Case 2
GM E-log: Case 2 : by M. Sai Anudeep R.no 98
CASE : 23 yr old male with B/L lower limb Paraparesis
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
After going through the patient details as given by our Intern Mam through the following link..
https://vaish7.blogspot.com/2020/05/medicine.html?m=1
My analysis of the patient is as follows :
Chief Complaints :-
1)weakness of bilateral lower limbs and complaints of tingling and numbness.
2)vomitings 5days back 3-4 episodes non projectile non bilious food particles is content.
3)when he got up for urination,suddenly he had a fall and got up with the help.
4)gluteal abscess since 5months ( operated 5 months back )
5)scrotal abscess since 20 days (incision and drainage 10 days back)
These two abscess are cold abcess
These two abscess are cold abcess
Weakness of B/L lower limbs :
Onset :sudden in onset
Duration :since 5 days
Associated conditions : Tingling and numbness
There is H/O sudden fall while he got up for urination and got up with the help of father.
The following are few causes for sudden fall are : Stroke , Infract , Ischemia
By evaluation and by complete detailed history pertaining to fall with relevant investigation can give the cause of the fall
Some Differentials for Paraparesis:
Infections causing lesions : Neurosyphillis is one of it , but here there will be progressive development in the symptoms where here it is sudden onset
Here neurosyphllis can be thought as the patient have multiple sexual partners.
But in history and examination no signs of primary syphilitic lesions
Traumatic lesions : can be ruled out here as there is no H/O of trauma
Infections causing lesions : Neurosyphillis is one of it , but here there will be progressive development in the symptoms where here it is sudden onset
Here neurosyphllis can be thought as the patient have multiple sexual partners.
But in history and examination no signs of primary syphilitic lesions
Traumatic lesions : can be ruled out here as there is no H/O of trauma
Vit-B 12 deficiency: on examination there is no pallor noted so this can be ruled out
Peripheral Vascular Disease: by history : no pain and claudications
On examination : no skin changes
So this can be eliminated from the differentials
Multiple Sclerosis: the mode of sudden onset will eliminate this
Neuro-muscular problem : on examination
Cns conscious
speech-normal
cranial nerves intact
MOTOR SYSTEM
Right Left
Bulk: Normal Normal
Tone: UL Normal Normal
LL Hypotonia Hypotonia
Power Right Left
Ul 5/5 5/5
LL 2/5 0/5
Reflexes.
Superficial reflexes
Right. Left
Corneal. P P
Conjunctival P P
Abdominal. P P
Plantar Extensor Extensor
Deep tendon reflexes
Right Left
Biceps 2+ 1+
Triceps 2+ 1+
Supinator 3+ 2+
Knee 3+ 2+
Ankle 3+ 2+
jaw jerk 1+ 1+
ankle clonus present absent
Primitive reflex -absent
Involuntary movements - absent
SENSORY SYSTEM - normal
CEREBELLUM
titubation - absent
Nystagmus- absent
Intensional tremors - absent
Pendular knee jerk - absent
Coordination test -normal
MENINGIAL SIGNS
Neck stiffness - negative
Kernigns sign - negative
Brudzinkis sign - negative
From the Nervous system examination mentioned above it is evident that there is
•B/L Hypotonia, Suggestive of LMN lesions
•Hyper reflexia of Knee and Ankle reflex suggestive of lesion UMN lesion above L3,L4
• Ankle clonus, suggestive of UMN lesion above S1,S2
Imaging :
 Spine and Abdomen X-ray
Spine and Abdomen X-ray 
Findings : multiple nodules in pulmonary apices suggest of pulmonary kochs and disseminated tuberculosis.





Findings : There are ring enhancing lesions and these can be Tuberculoma
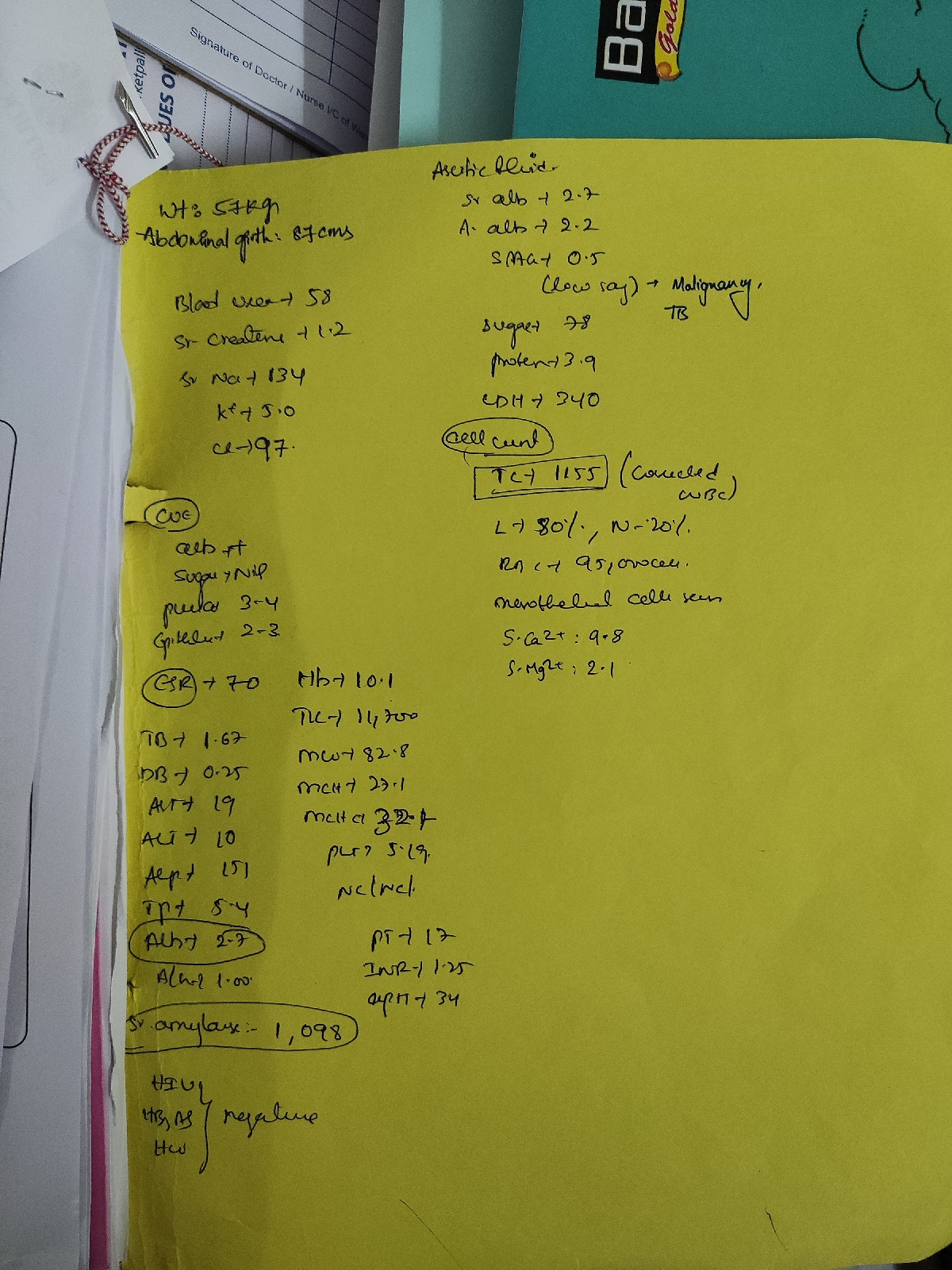
Abnormalities found in LFT : SGOT (AST) : 80 IU/L (NORMAL: <40 IU/L)
Alkaline Phosphate 192 IU/L ( NORMAL : 4O TO 129 IU/L )
Vomiting :
It may be be due to intra cranial space occupying lesions ( here it may be due to a Tuberculoma or any other ICSOL)
Anatomical Location :
Anatomical location of present Ring enchancing lesions lies in the anterior right and left cerebral hemispheres, midline of falx cerebri and pyramidal tracts .
Features of both UMNL and LMNL are seen
Features in favour of UMNL : Ankle clonus
Features in favour of LMNL : Hypotonia
The lesion is most probably at L3 and L4
Pathologically :
Pathologically the cause can be due to Clod abscess caused by MTB extending to L4 L5
Biochemical Abnormalities:
Due to lesions in Brain there are elevated AST levels
Provisional Diagnosis
Paraparesis with L4,L5infective spondylodiscitis with left psoas abscess with ring enhancing lesions in right and left cerebral hemispheres with healing ulcer in right gluteal region secondary to drained gluteal abscess with pyocele left side operated ( 10 days back)
Treatment Plan :
Anti Tuberculosis Treatment ( Pyridoxine is given to prevent neuropathy caused by isoniazid
Taylars Brace for 18-24 months with adequate rest and frequent change in positions
My thoughts in this case :
We found that patient have TB incidentally
As The patient have multiple sexual partners it is to screen him for HIV as TB and AIDS are commonly go hand in hand
And it is advised to do RTPCR for knowing any resistant strain of Myocobacterium
And also do screening of HIV for his sexual Partners
Patient is having Dissiminated TB it may spread and cause abscess at right gluteal region and scrotal region
Cold abscess formed may compress at L4 and L5 causing Paraparesis
There are ring enhancing lesions which might be Tuberculoma
There are both UMNL and LMNL which needs detailed investigation
And detailed history of Fall when got up for urination to be evaluated thoroughly
CT spine to be done for elimination of Potts spine
My references
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208909/
My Questions
1. Does these lesions Shown in MRI may cause his symptoms
2. What effects of compression due to abscess may occur
3. Pathway of spread of M.bacterium to Brain and gluteaus
4. What might caused scrotal abcess